Radical Client Centred (RCC) Framework
For Disordered Eating/ Eating Disorders (DE/ED)
Dr Christie Bennett and Josephine Money ©2025
Download PDF- RCC
Download PDF- RCC worksheet PDF
"If I could get up in the middle of an eating disorder conference and say one thing, it would be, all of you, just stop, listen; the most reliable source of evidence is the client sitting in front of you."
As practitioners supporting clients with eating disorders we are afforded the great privilege of holding space for and bearing witness to our clients healing. It takes courage to seek help, be open, honest and vulnerable in their exploration and experimentation towards change.
Disordered eating/eating disorders (DE/ED) do not develop in isolation. There are complex interrelationships between biological, social, cultural and psychological factors that contribute to the development and maintenance of disordered eating/ eating disorders (DE/ED)(1). However, dietetic understanding, acknowledgement and confidence of addressing these factors in practice is low (2). Therefore, we set out to partner with lived experience to create a resource for use by dietetic and other health professionals working with clients with DE/ED.
Lived experience experts with a range of marginalized identities participated in paid interviews exploring their experience of DE/ED and accessing support. Thematic analysis of interview transcripts was undertaken. Results are presented as a visual framework entitled ‘The Radical Client Centered (RCC) Framework©’. The aim of this resource isto assist in formulation of the impact of cultural constructs and systemic oppression for individuals on the development and relationship of DE/ED.
The Radical Client Centered (RCC) Framework provides a visual tool to prompt reflection on the multiple systemic, interpersonal and intrapersonal systems that may lead someone to a rupture in their relationship with food and body. In turn, this rupture in the relationship between food and body can lead to the development of disordered eating or an eating disorder (DE/ED). This is our invitation to listen more and speak less (3) and learn from our clients the way these factors have impacted the development of their DE/ED.
Further, we encourage a reflection on the healing power of allowing people the space to share and hear their own narrative of their body story (4). There are few places that people are afforded the space to explore their relationship with food and body, particularly across the timeline of their life. This process may be an important part of the assessment and building of therapeutic alliance before embarking on evidence based treatments (EBT).
In supporting people to heal from DE/ED try to understand the presenting symptoms and behaviors, in the context of the person's history, social context and life goals. Further, we encourage all practitioners to take the time to empathise, validate, appreciate the nuance in their experience and the levels of harm and disconnect that may have occurred.
This reflective tool provides a framework to consider in session with the client or in supervision, the impact of the client's experiences in each domain and what may need to be considered, validated, explored and navigated to support understanding and support.
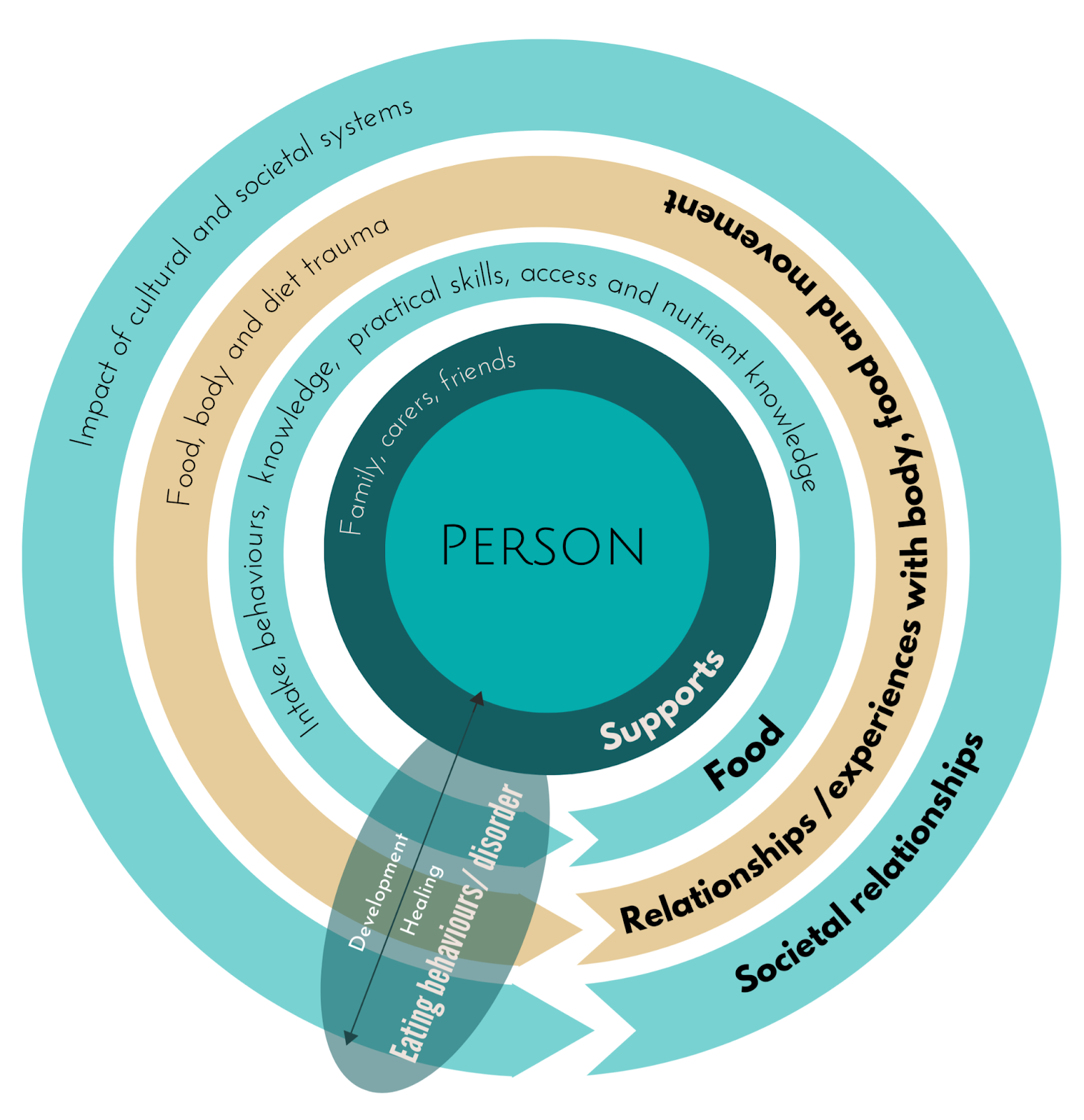
The Framework:
The RCC Framework is a diagram of concentric rings echoing from the central individual. Each circle represents a domain to be considered in the development and healing of their ED/DE This individualisation is an essential step forward in improving consumer outcomes for individuals with DE/ED as is a priority for future research (5).
Below we speak to each domain and how it may intersect and the implications for formulation and treatment. Where you see italicized font, these are direct quotes from our paid lived and living experience consultants. We have selected these quotes as examples of the themes that occurred in the interviews. All consultants have had the opportunity to review the framework and quotes before publication.
"I don't feel it's fair for a whole lot of people that do have lived experience, because we shouldn't have to legitimize our experience through academia. That's part of the institutional power that academia has. And, unfortunately, again, that's upheld by the eating disorder community, they see high quality peer reviewed research in the Journal of eating disorders, for instance, as more reliable to put it bluntly, as a person with lived experience in a bigger body, who has had a pretty shocking time throughout treatment.
I am always seen as a less reliable source of evidence of my own experience because I don't have an academic back catalog. I don't have 20 odd years of clinical experience behind me. All I have, and I hate to say, all I have is knowledge and experience. And unfortunately, this is part of the problem."
The Person
Identities
"I just think that there's such a, there's just such a lack of awareness in the eating disorder field, when it comes to people experiencing aspects of their identity as a collective, as opposed to individual compartmentalizing parts of ourselves. I'm part of the queer community, I'm neurodivergent, I have a chronic illness, you know, I don't experience those things in silos independent of one another, I experienced those aspects of my identity collectively, that's who I am.”
The first consideration in this theme is that all clients are individuals with unique experiences. There will be similarities in the way that people’s DE/ED presents. Similar themes that may have contributed to development and triggered the DE/ED. There will be similar intervention approaches that assist in making change. However, no two people will have the same experience. No two people with DE/ED will have the same origins story. We need to consider that individuals hold many intersecting identities. These identitieshave an influence on the relationships with food, body and movement from a very young age. All people with DE/ ED will have different signs, symptoms, behaviors and experiences and their process in healing will therefore be unique.
What about the evidence we hear you say? The evidence should always be part of the clinician's consideration, not the entire manual. By this we mean, consider the evidence within the context of the individual's experience, values and your clinical judgement. In the literature this is referred to as the three legged stool (6,7). In this it is important to consider that the process of uncovering and accepting our individual identities and these being respected and accommodated has a significant influence on a person's experience.
"You don't need to fix everything, but you (dietitians/health care professionals) do need to acknowledge the interrelationships of intersectional identities "
"we're living in this broken world, we're living in a world that doesn't make room for people. We're living in a world that, you know, essentially pushes people further and further into the margins. We're living in a world that's completely inaccessible for a lot of people."
There is an increased incidence of DE/ED for people with marginalized identities including queer, sexual and gender minorities (8-12) neurodivergent (13-17), gender non conforming, non binary and trans populations (18,19), disabled people (20-26), people in fat and higher weight bodies (27), black, Indigenous and People of Colour (BIPOC) (28,29).
In conjunction with the societal relationship, these identities are not always acknowledged, understood, honored or nurtured. The person may have experienced discrimination, stigma and trauma as a result of their identity. This trauma may further disconnect them from their authentic selves. This oppression can lead to dysregulation within the individual (30) and the DE/ED may develop in an attempt to assimilate to the dominant socially acceptable identities, or to self soothe via nervous system regulation.
Finally, there is an increased incidence of DE/ED with some medical conditions including but not limited to diabetes, PCOS and cystic fibrosis. If these diagnoses are considered within the context of the We typical weight centric western medical system. It is understandable that the often rigid, weight based interventions, echoing diet culture; this can cause decreased trust and connection to the body. Therefore, this may need to be explored and validated for the person. This may take time, as rebuilding trust in the medical system may require significant healing.
If you are an allied health practitioner it is not in your scope to diagnose or provide intervention in relation to all aspects that are uncovered when exploring a client's individual experience. However, it is within all health professionals scope and remit to listen, validate and assist clients to connect with the right practitioner when needed.
"(Practitioners) need to acknowledge the power in validating"
Supports
The social support that an individual has access to, or lack thereof, may have contributed to the development of the DE/ED and may be a key factor in their healing. The RCC Framework asks practitioners and clients to consider the supports available to them. This might be family of origin or family of choice. Further, community can be important for people who hold identities that are often oppressed in our cultural context. Being able to see, connect and have relationships with others who we can see ourselves in is validating. The impact of these supports cannot be underestimated and hence a whole section of the framework has been dedicated to this.
"(the power of) Seeing, celebrating, and existing in community"
Food
Intake, behaviors, knowledge, practical skills, access, nutrient knowledge
Food can be such an emotive word and is a wide encompassing topic. Food is a key part of many cultural and religious rituals and this may have shaped people's perception and relationships with particular foods and the rituals around them. However, there may be interpersonal distress and traumas related to these celebrations, that occur when people are connected with a wider family and are therefore associated with these foods moving forward.
This is a good example of the ‘Three Legged Stool’ previously discussed. As practitioners we need to acknowledge the literature but also be cognisant and responsive to cultural factors that may alter the expectations for change, pace or what recovery may look like for each individual.
Further, knowledge and understanding of nutritional value of food may be influenced by diet culture, leaving people misled and confused. During ED/DE treatment may be the first time these long held (often culturally accepted) beliefs are challenged. Understandable, we can expect resistance to unlearning and relearning and need to compassionately and patiently allow time for this.
Importantly, it is important not to t assume people's skills in food acquisition and preparation. There may be barriers that make this difficult such as financial, environmental or heightened sensory sensitivity making shopping difficult. Unrealistic cultural expectations of cooking from scratch and healthism beliefs can be a barrier to using readily available short cuts for food preparation such as meal delivery services, pre-cut or frozen vegetables. When exploring how the DE/ED presents for someone, we need to consider so much more than their actual intake. We can not assume someone's knowledge, skills and access to foods when supporting them in recovery.
Relationships and experience with body, food and movement
Many individuals we support have experienced diet, movement and body trauma where the innate connection with these parts of self has become ruptured and lenses of trauma have clouded the perception of these important internal relationships. In most cases, it is safe to assume that if there is DE/ED there is also diet and body trauma to explore.
Body trauma
Body trauma may be any experience that has caused distress for the person around the function or aesthetic of their body. This may occur at the interpersonal level - internalizing cultural messages regarding idealized bodies, desirability, and healthism that someone feels their body does not meet these ideas and needs to be altered, corrected or fixed in some way (4). People in disabled bodies or higher weight bodies receive constant messaging from our culture that their bodies are not acceptable in the way that public spaces are not set up to accommodate them.
This can also occur at an intrapersonal level and systemic level where someone is told that their body is inadequate, incorrect and/or needs fixing. An example of this, pertinent to the ED field as we know that people in higher weight bodies develop DE/ED at a higher incidence (26,31-38). Compounding this,is people in a higher weight body who experience anti fat bias in medical spaces, microaggressions with peers and living in a physical world that is not built to accommodate their body.
These feelings may present cognitively as negative thoughts regarding the body, decreased sense of self worth as a result of not meeting these expectations or decreased self confidence in social interactions. As with many things, the intensity of these thoughts will exist on a spectrum. An example of this spectrum might be where the feelings are like background noise that the person can ignore and disengage from, right through to intrusive thoughts the person feels unable to disengage from and impact on their daily functioning.
The distress of body trauma d may lead to engaging in behaviors to alter the body. This may include an adjustment in foods consumed or the activities the person engages in with the purpose of changing the body shape or size. These behaviors can overlap with traditionally held ideas of ‘healthy’, ‘healthful’ or ‘health seeking’ behaviors. We need to be aware that the motivation behind these behaviors and the compulsion to engage in them sets this apart from being a self care behavior to actually being self harming behaviour. However, this can also be informed by advice from healthcare professionals and hence further driving the want to be ‘accepted’ by others, especially those in positions of authority.
Body trauma may also occur at the interpersonal level. This is where other people make comments about an individual's body. This comment may be intended as positive, but have a negative impact that the person feels they need to maintain the current functionality or aesthetics of their body to be acceptable, valued or desirable. Or, it may be direct negative feedback about the aesthetics, functionality or implied acceptability or health of someone's body.
People in disabled bodies or higher weight bodies receive constant messaging from our culture that their bodies are not acceptable in the way that public spaces are not set up to accommodate them. Therefore, this may be an important component in the development of the person's ED/DE that may need to be unpacked.
Diet trauma
Diet trauma may present as the dysregulation and distress that can arise from past experience with change from an innate drive to eat to an external locus of control. This might include rigid food rules, restriction, cognitions or beliefs around food, food insecurity or deliberate external control of food availability or access. This deliberate change to eating patterns, once or many times, may leave an individual feeling they can not trust their internal preferences or wisdom around nourishing themselves.. Individuals may have a strong internal response or resistance to talking about food or direction to change food patterns. Often the reason why this discomfort exists is not immediately obvious. This can be deeply ingrained that people are often unaware of this psychological deprivation until they are exploring it as part of their DE/ED recovery. For example, when exploring the drive to binge eating, people are often frustrated that they are eating regularly, are not physically hungry, using alternative coping strategies and yet still feel the compulsion towards previously ‘bad’ foods. The trauma of avoiding these foods for so long or chastising themselves for so long, needs time to be explored and healed to truly feel all food is neutral and acceptable as part of their dietary intake. This can be an invitation to lean in and be curious about past experiences with diet manipulation and allow people time to explore this, validate their experience and more fully understand it before launching into providing dietary recommendations.
Inability to comply with the innate drive often is informed on some level to an attempt to comply, adapt or assimilate more easily; or as a direct result of external pressure from peers or health practitioners. There is often a differential of power in health spaces and individuals may feel there is no option but to comply with directives. There may be pressure to drop cultural food practices, ignore sensory safety with food or restrict intake with the purpose of shrinking the body. As practitioners, it is increasingly important we are aware of the imbalance and allow opportunities for the person to understand they are the expert of their experience.
Movement trauma
Like diet and body trauma movement trauma or a disruption in the innate relationship between the body and movement can occur during episodes of ED/DE. A disruption in this relationship can look like an increased drive to move regardless of illness, nourishment, pain or injury. Further, it could also be an association between movement and body changes. Understanding the history and current relationship with movement can be a key piece of information to move forward in your treatment or formulation with a client. Note that this conversation, like body and food trauma, may take time. It may require some uncomfortable reflection or uncovering subconscious beliefs for the client. Stay patient, present and curious through the discomfort.
"Hear and believe the person They have the best knowledge of themselves"
Societal Relationships; Impact of cultural systems.
”You can't expect us to thought challenge or behavioral experiment ourselves out of systemic oppression!”
Interwoven through the inescapable cultures we are encompassed within are many systems of inequality and oppression that have a significant impact on the individuals we support and the development of their DE/ED. We can not consider an individual, the function that the DE/ED serves for them and the most helpful steps forward without appreciating the wider systems that have impacted its development.
These sociocultural systems intersect and impact the relationship an individual develops with their bodies and food. When people are impacted by multiple systems of inequality rather than having a cumulative impact these “intersecting systems of inequality produce new and complex patterns of advantage and disadvantage” (3).
Some social cultural systems to consider that may have impacted an individual's mental health and relationship to food and body may include (3):
-
Racism
-
Patriarchy
-
Settler Colonialism
-
Ableism
-
Ageism
-
Classism
-
Neuronormative
-
Cisgenderism or Cisnormativity
-
Heterosexism
-
Religion
-
Anti Semitism
-
Socioeconomic advantage
-
Anti fat bias/Sizeism/Fatphobia
-
Diet culture
These systems of inequality that exist may lead to experiences such as:
-
Systemic oppression of marginalized groups
-
Systemic, interpersonal and intrapersonal bias and discrimination
-
Trauma, abuse and bullying
-
Health inequality and limited access to adequate health care
-
Limited access to safe and consistent food and water
It may or may not feel appropriate to have discussion with each individual client about their experiences within cultural systems but it is important as practitioners that we take the time to learn from people who have experienced disadvantage as a result of systemic inequalities.
There will be some systems of inequality that practitioners as individuals are disadvantaged within and others we are privileged within. It is important for practitioners that we are aware of our status with these systems. Stephaine Nixon in her Paper introducing ‘The Coin Model of Privilege and Critical allyship in Health’, shares a reflection that is a poignant invitation to do just that:
“I seek to understand my own roles in upholding these systems of inequality.
I seek to learn from people at the bottom of the coin. If I'm going to work with folx from the bottom of the coin it's not as the expert that's going to help them, it's working in solidarity with them so that we can all be dismantling the coin”(3).
A note on 'Recovery'
" I mean, can you really put an overarching definition of recovery, for every person with an eating disorder? I don't think so. It means different things to different people"
We need to be aware of the language we use with clients and hold space to explore what recovery or improvement means to them. The term 'recovery' has connotations of a defined destination whereby they conform to societal norms and cultural hegemony.
When considering the oppressive cultural systems at play, we need to remember that these are unlikely to shift in a client's lifetime and thus the harm of these will continue. Some level of DE/ED or associated cognitions may continue as a result of this; and this is not in an individual's control. However, this does not mean that their quality of life, safety and health can not improve. We need to ensure that we are collaborating with clients to determine what meaningful change looks like for them and what is achievable.
For example, if we consider the spectrum of eating that we often discuss with clients we may present a double ended arrow with “normal eating” at one end and EDs at the other. ‘Normal’ is a subjective, nuanced and individual concept. Definitions of ‘normal eating’ often include themes of attunement to the physical body, innate knowledge and access to adequate nutrition. Therefore, ‘normal’ eating will look different for everyone and that it is not simply eating three meals and three snacks per day. By upholding these rigid standards of eating expectations, we risk further harm as we set up the client for an unrealistic goal. Assumptions that all people will be able to safely connect to their body, trust it or even have interoception skills is ableist and neuronormative and ignores the possibility of ongoing experiences of trauma preventing people from feeling safe to connect with their bodies.
An alternative may be to discuss with individual clients what they would like to focus on and would interpret as meaningful change. This could be defined as neutral, enjoyable, calm, safe or happy eating. In our course, “I've done the basic training; Now what?” Intermediate skills in supporting individuals with eating disorders, we propose an alternative definition: “Eating in a way that is most affirming and relaxed for my needs. Knowing that this supports my emotional regulation and nutritional needs. Able to be flexible, spontaneous and social with food if this is something that respects my neurodiverse needs” (39).
" I guess personally, for myself I don't ever see myself as being recovered, I see myself in a constant state of recovery. And I think, given the fact that there's so much, you know, systemic oppression when it comes to fat phobia, when it comes to sexism, when it comes to homophobia, transphobia, racism, ableism, neuro normativity, that sort of thing; when there's so much systemic oppression.
And historically, eating disorder treatment has never actually incorporated this; how do we expect people to reach this arbitrary point of recovery, when we're not actually addressing the systems of harm and the systems of oppression that go on to affect people's lives on the daily? You know, it's like asking people to, I don't know, like, compartmentalize themselves, it's like, can we just put your trauma aside? And focus on this tiny part of yourself ?"
Using the RCC framework
There are a range of ways that this framework can be utilised in supportive and clinical work with individuals experiencing DE/ED.
The RCC Framework is a visual tool that offers an opportunity to consider the individual's experience of DE/ED from a more personalised perspective; considering many of the factors that have contributed to the development of DE/ED and are important to be aware of in the process of recovery.
The RCC was informed by our lived experience interviews which highlighted the importance of taking the time to connect with the individual and their experience of DE/DE. Further, our lived experience experts and the literature strongly emphasize how this connection can have a positive impact on the therapeutic alliance and the efficacy of ED intervention.
This is a tool that practitioners can use in the therapeutic space. It is designed to be used with the client during assessment and formulation to allow a deeper understanding of the client's experience. Further, it allows the individual to have an opportunity to build a narrative around their own experience is in itself healing, such as in narrative medicine. A strength of this tool is that it encourages a shift to empower clients to correctly reallocate anger and frustration to the system of inequality and other experiences in their life that they may not be aware of or be able to control rather than at themselves.
We also encourage the RCC to be used to improve the reflective skills and reflexivity of practitioners. It might be helpful to take this tool to supervision when a practitioner is feeling stuck. The frameworkhighlights not just the personal experience of a DE/ED, but the predetermined and precipitating systemic and interpersonal factors that are critical consideration in this work. It is designed to give practitioners permission to slow down and hold space to validate the client's experience while allowing further exploration of the relationships in the systems they exist within.
Byrne and Fursland invite exploration and “embracing of new knowledge, treatment approaches and cultural shifts” in response to patients and families requesting more individualized care (5). The RCC is proposed as a framework for further exploration, revisions and rigorous testing that may assist in assessment, formulation, treatment planning of current EBT with adaptations based on individual presentations.
"The homogeneity of the dietitian industry and how it is typical white, smaller body, middle class women who are in that industry; I kinda feel like, you see this alot with you know cis gender hetrosexual white people; they don't have marginalized experiences. Often those in smaller or thin bodies have, they never had to confront some of the things that those of us with marginalized experiences have.
If people are going into these careers thinking I'm just going to help people achieve their body goals. If that is all you think you are going to get out of your career and that's as hard as it's going to get -helping someone to stick to their diet - then i think that is a really harmful attitude to bring in to this industry.``
References:
1. Frank GK. The Perfect Storm - A Bio-Psycho-Social Risk Model for Developing and Maintaining Eating Disorders. Front Behav Neurosci. 2016 Mar 10;10:44. doi: 10.3389/fnbeh.2016.00044. PMID: 27014006; PMCID: PMC4785136.
2. Heafala A, Ball L, Rayner J, Mitchell LJ. What role do dietitians have in providing nutrition care for eating disorder treatment? An integrative review. Journal of Human Nutrition and Dietetics. 2021 Aug;34(4):724-35.
3. Nixon, S.A. The coin model of privilege and critical allyship: implications for health. BMC Public Health 19, 1637 (2019). https://doi.org/10.1186/s12889-019-7884-9
4. Kinavey, H. (2022). Reclaiming body trust: A path to healing & liberation. Unabridged. New York, Penguin Audio.
5. Byrne, S.M., Fursland, A. New understandings meet old treatments: putting a contemporary face on established protocols. J Eat Disord 12, 26 (2024). https://doi.org/10.1186/s40337-024-00983-4
6. Peterson CB, Bleck Becker C, Treasure J, Shafran R, Bryant-Waugh R. The three-legged stool of evidence-based practice in eating disorder treatment: research, clinical, and patient perspectives. BMC Med. 2016. https://doi.org/10.1186/s12916-016-0615-5.
7. Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn’t. BMJ. 1996;312(7023):71–2.
8. Parker LL, Harriger JA. Eating disorders and disordered eating behaviors in the LGBT population: a review of the literature. J Eat Disord. 2020;8(51):1–20. https://doi.org/10.1186/s40337-020-00327-y.
9. Nagata JM, Ganson KT, Austin SB. Emerging trends in eating disorders among sexual and gender minorities. Curr Opin Psychiatry. 2020;33(6):562–7.
10. Calzo JP, Blashill AJ, Brown TA, Argenal RL. Eating disorders and disordered weight and shape control behaviors in sexual minority populations. Curr Psychiatry Rep. 2017;19(8):49. https://doi.org/10.1007/s11920-017-0801-y.
11. Mensinger JL, Granche JL, Cox SA, Henretty JR. Sexual and gender minority individuals report higher rates of abuse and more severe eating disorder symptoms than cisgender heterosexual individuals at admission to eating disorder treatment. Int J Eat Disord. 2020;53(4):541–54.
12. Dufy ME, Henkel KE, Earnshaw VA. Transgender clients’ experiences of eating disorder treatment. J LGBT Issues Couns. 2016;10(3):136–49.
13. Baraskewich J, von Ranson KM, McCrimmon A, McMorris CA. Feeding and eating problems in children and adolescents with autism: a scoping review. Autism. 2021;25(6):1805–1519.
14. Baraskewich J, Climie EA. The relation between symptoms of ADHD and symptoms of eating disorders in university students. J Gen Psychol. 2022;149(3):405–19. https://doi.org/10.1080/00221309.2021.187486.
15. Levin RL, Rawana JS. Attention-deficit/hyperactivity disorder and eating disorders across the lifespan: a systematic review of the literature. Clin Psychol Rev. 2016;50:22–36. https://doi.org/10.1016/j.cpr.2016.09.010.
16. Villa FM, Crippa A, Rosi E, Nobile M, Brambilla P, Delvecchio G. ADHD and eating disorders in childhood and adolescence: an updated minireview. J Affect Disord. 2023;321:565–271.
17. Yao S, Kuja-Halkola R, Martin J, Lu Y, Lichtenstein P, Norring C, Birgegård A, Yilmaz Z, Hübel C, Watson H, Baker J, Almqvist C, Eating Disorders Working Group of the Psychiatric Genomics Consortium, Thornton LM, Magnusson PK, Bulik CM, Larsson H. Associations Between Attention-Deficit/ Hyperactivity Disorder and Various Eating Disorders: A Swedish Nationwide Population Study Using Multiple Genetically Informative Approaches. Biological Psychiatry. 2019; 86:577–586
18. Keski-Rahkonen A. Eating disorders in transgender and gender diverse people: characteristics, assessment, and management. Curr Opin Psychiatry. 2023;36(6):412–8. https://doi.org/10.1097/YCO.0000000000000902.
19. Simone M, Hazzard VM, Askew AJ, Tebbe EA, Lipson SK, Pisetsky EM. Variability in eating disorder risk and diagnosis in transgender and gender diverse college students. Annals of epidemiology. 2022 Jun 1;70:53-60.
20. Gravestock S. Eating disorders in adults with intellectual disability. J Intellect Disabil Res. 2000;44(6):625–37.
21. Hove O. Survey on dysfunctional eating behavior in adult persons with intellectual disability living in the community. Res Dev Disabil. 2007;28:1–8.
22. Schilder CMT, van Elburg AA, Snellen WM, Sternheim LC, Hoek HW, Danner UN. Intellectual functioning of adolescent and adult patients with eating disorders. Int J Eat Disord. 2017;50:481–9.
23. Kothari R, Solmi F, Treasure J, Micali N. The neuropsychological profile of children at high risk of developing an eating disorder. Psychol Med. 2013;43:1543–54. https://doi.org/10.1017/S003329171200218.
24. Lopez C, Stahl D, Tchanturia K. Estimated intelligence quotient in anorexia nervosa: a systematic review and meta-analysis of the literature. Ann Gen Psychiatry. 2010;9:40–40.
25. Smith B, Rogers SL, Blissett J, Ludlow AK. The relationship between sensory sensitivity, food fussiness and food preferences in children with neurodevelopmental disorders. Appetite. 2020;150:104643–104643.
26. Smith B, Gutierrez R, Ludlow AK. A comparison of food avoidant behaviours and sensory sensitivity in adults with and without Tourette syndrome. Appetite. 2022;168:105713–105713.
27. Ralph, A.F., Brennan, L., Byrne, S. et al. Management of eating disorders for people with higher weight: clinical practice guideline. J Eat Disord 10, 121 (2022). https://doi.org/10.1186/s40337-022-00622-w
28. Taylor JY, Caldwell CH, Baser RE, Faison N, Jackson JS: Prevalence of eating disorders among Blacks in the National Survey of American Life. Int J Eat Disord. 2007, 40 Suppl:S10-4. 10.1002/eat.20451. https://onlinelibrary.wiley.com/doi/epdf/10.1002/eat.20451
29. Burt A, Mitchison D, Dale E, Bussey K, Trompeter N, Lonergan A, Hay P. Prevalence, features and health impacts of eating disorders among First-Australian Yiramarang (adolescents) and in comparison to other Australian adolescents. J Eat Disord. 2020;8:10–10. https://doi.org/10.1186/s40337-020-0286-7.
30. Sherin JE, Nemeroff CB. Post-traumatic stress disorder: the neurobiological impact of psychological trauma. Dialogues Clin Neurosci. 2011;13(3):263-78. doi: 10.31887/DCNS.2011.13.2/jsherin. PMID: 22034143; PMCID: PMC3182008.
31. Duncan AE, Ziobrowski HN, Nicol G. The prevalence of past 12-month and lifetime DSM-IV eating disorders by BMI category in US men and women. Eur Eat Disord Rev. 2017;25:165–71.
32. Sawyer SM, Whitelaw M, Le Grange D, Yeo M, Hughes EK. Physical and psychological morbidity in adolescents with atypical anorexia nervosa. Pediatrics. 2016;137(4):4080. https://doi.org/10.1542/peds.2015-4080.
33. Lavie CJ, De Schutter A, Milanet RV. Healthy obese versus unhealthy lean: the obesity paradox. Nat Rev Endocrinol. 2015; 11: 55–62 https://doi.org/10.1038/nrendo.2014.16
34. Hart LM, Ferreira KB, Ambwani S, Gibson EB, Austin SB. Developing expert consensus on how to address weight stigma in public health research and practice: a Delphi study. Stigma Health. 2020;6:179–89.
35. Vartanian LR, Porter AM. Weight stigma and eating behavior: a review of the literature. Appetite. 2016;102:3–14.
36. Puhl RM, Luedicke J, Grilo CM. Obesity bias in training: attitudes, beliefs, and observations among advanced trainees in professional health disciplines. Obesity (Silver Spring). 2014;22(4):1008–15. https://doi.org/10.1002/oby.20637.
37. Mensinger JL, Tylka TL, Calamari ME. Mechanisms underlying weight status and healthcare avoidance in women: a study of weight stigma, body-related shame and guilt, and healthcare stress. Body Image. 2018;25:139–47.
38. O’Brien KS, Latner JD, Puhl RM, Vartanian LR, Giles C, Griva K, Carter A. The relationship between weight stigma and eating behavior is explained by weight bias internalization and psychological distress. Appetite. 2016;102:70–6.
39. Money and Bennett (2023). “I've done the basic training; Now what?” Intermediate skills in supporting individuals with eating disorders. Teachable. Available at: https://elleducation.teachable.com/p/conceptualising-eating-disorders.